

Gallstones & Cholecystectomy
How do I know I have gallstones?
The type of pain caused by gallstones is called biliary pain. Its characteristics are as follows:
Nature: Steady (not colicky or windy pain)
Intensity: Severe enough to inferfere with your activity
Location: Upper abdominal pain (may be in the chest and back/shoulder blade)
Duration: Not less than 15 minutes, usually 1 to 5 hours
Onset: Rapid
Relief: Not relieved by household remedies, position change or passage of wind
Frequency:Usually episodic and infrequent rather than continuous
Timing: May occur after food. Often wakes people at night (usually in the early hours of the morning).
Belching, bloating and fatty foods intolerance occur equally often in those with and without gall stones.
Gallbladder Surgery
Laparoscopic cholecystectomy is the complete removal of the gall bladder without a major abdominal incision. Cholecystectomy is the surgical removal of the gallbladder and laparoscopic refers to the type of instrumentation and procedure used for this operation.
The procedure is performed in the operating room while the patient is under a general (complete) anaesthetic. Four small 5-10 mm incisions are used, one at the umbilicus (belly button), through which the laparoscope is inserted into the abdomen. Three punctures along under the ribs are used for placement of the instruments for removing the gallbladder and an additional tiny wound may be made for taking x-rays if necessary.The laparoscope is a long, narrow instrument consisting of a lighted tube with magnifying lenses – to serve as a surgical viewing scope. It is attached to a small television camera in order for the surgeons and all assistants to view the gallbladder on an external video monitor during the procedure.
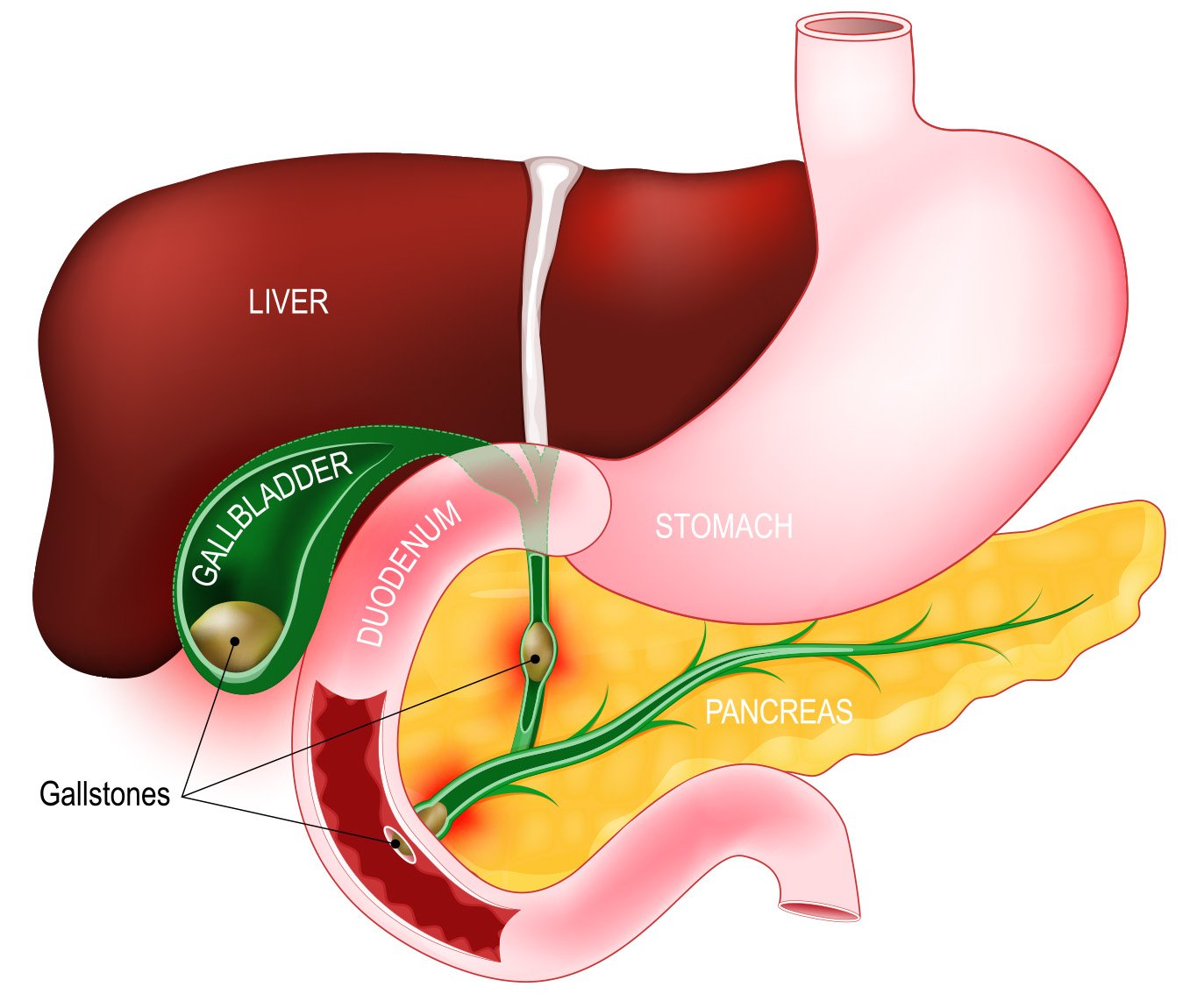
The gallbladder is a sack attached to the underside of the liver, which stores bile. There are two major vessels attached to the gallbladder; the cystic artery which supplies blood to the gallbladder, and the cystic duct which transports bile to and from the bladder.
Either plastic or metallic surgical clips are placed on the duct and artery leading to the gallbladder, in order to secure the structures against leakage or bleeding. Then an instrument heated by electric current is used to cut the attachment of the gallbladder from the liver bed. The gallbladder is then removed from the abdominal cavity through the incision in the umbilicus. This incision may be enlarged slightly if the gallstones are large. The time required to complete the procedure varies from 25 minutes to 3 hours, depending on the state of the gallbladder, the amount of inflammation or swelling present and the local anatomy.
94-97 of every 100 patients will be cured of their pain after laparoscopic cholecystectomy. The complications of gallstones will be prevented.
Why is the Procedure Performed?
Any cholecystectomy is performed when your doctor concludes that the gallbladder is diseased, not functioning properly and/or contains gallstones. The gallbladder is removed to avoid further complications such as bile duct obstruction, which can affect the liver. Indications for surgery include:
Any patient with a complication of gallstone disease.
Any patient with uncomplicated symptomatic gall stone disease who has had the natural history of symptomatic gallstones explained to them, and makes an informed choice to have surgery.
Asymptomatic gallstone patients with a calcified gallbladder or a gall bladder polyp greater than one centimetre in diameter
Selected asymptomatic diabetic patients with gallstones
The laparoscopic method of cholecystectomy is performed as a way to avoid, if possible, the major abdominal incision required for other methods of gallbladder removal, as well as to have minimal bleeding during the operation process. The major abdominal incision in regular gallbladder removal procedures is the principle cause of the extended recovery period required.
Converting to Open Procedure during the Laparoscopic Cholecystectomy
In some cases, circumstances may arise during the procedure which may cause the surgeon to abandon the laparoscopic technique in favour of an “open” cholecystectomy procedure performed through a standard incision. Some of the circumstances that may require conversion to open procedure include excessive bleeding, intense inflammation in the gallbladder or stones in the bile duct. The same anaesthetic is used, but the surgeons must make another type of incision and alter their methods of gallbladder removal.
Benefits/Advantages of Laparoscopic Cholecystectomy
The advantages to the patient derived from removing the gall bladder by the laparoscopic method, in contrast to other removal procedures are:
Reduced postoperative pain
Shorter hospital stay
Earlier return to full activity and work
Less pain medication requirement
Less visible abdominal scars
Risk involved in the laparoscopic procedure
The major risks associated with this procedure are similar to those with open cholecystectomy. These are infrequent or rare. The most common risks include:
Bleeding
Infection
Complications related to general anaesthetic (including the rare incidence of heart attack and death)
Injury to the bile duct which could require major reconstructive procedures
Blood clots forming in the legs
Leakage of bile from the bile ducts into the abdomen
Injury to abdominal organs from the laparoscopic insertion
Studies of laparoscopic procedures have found the following types of problems:
Complications: 3-8 people in every 100
Bile duct injuries: 1 in every 1000 people
Conversion to Open Procedure: 2-4 people in every 100
Deaths: 1 in every 1500-3000 people
Open operations may have a slightly lower rate of bile duct injuries and slightly higher rates of overall complications and deaths.
Alternative Treatments
Other methods for treatment of gall stones also exist. These methods include removal, dissolving or breaking up of the gall stones without gall bladder removal using:
Medications or chemicals to dissolve stones
Shock waves passed through the skin to break up stones (lithotripsy)
Unfortunately these treatments are not applicable to the vast majority of patients and are rarely practiced in Australia as they seldom work.
If only the gallstones and not the gallbladder is removed there is a high probability that stones will reform in the gallbladder and symptoms will continue or recur. (It is rare for gallstones to form again in the bile duct after cholecystectomy).
Long term consequences of gallbladder removal
For most patients there will be no long term side effects of having a diseased gallbladder removed. Once the wound pain has settled a very small number of patients may have more frequent bowel actions and some gastro-oesophageal reflux symptoms.
What will happen if I don’t have surgery for Gallstones?
Asymptomatic gall stones (If your gallstones are not causing you pain):
After gallstones are detected serious symptoms and complications will probably develop in 2 in every 100 people per year. This gets less common after ten years.
Biliary pain is the first symptom to develop in about 90% of people with previously asymptomatic gall stones. After 20 years, two thirds of patients with asymptomatic gallstones will have had no biliary pain or complications.
The lifetime risk of death with a wait and see approach is 0.8% to 2%. The risk may increase the older you are when your gall stones are detected.
Symptomatic gallstones (If your gallstones are causing you pain):
About 30% of patients who have an episode of biliary pain will not have further episodes of pain during the next ten years.
About 1-2 patients in every 100 develop complications of gallstones per year. After 20 years about half the patients with symptomatic gallstones will not have had a biliary complication.
The lifetime risk of death with a wait and see approach is 2% to 6%. The risk increases the older you are and when your gallstones are first detected.
General Surgery across Lake Macquarie, Newcastle, Hunter Valley, Gateshead
Our surgeons see both public and private patients in the Surgery Central consulting rooms in the Lake Macquarie Specialist Medical Centre and operate in both public and private hospitals.